Gait analysis has been used in the clinical setting to assist surgical planning in children with cerebral palsy for more than three decades, and with convincing results [1, 2]. Gait analysis observes the movement of the lower limbs in order to identify the underlying problems resulting in difficulties in walking for the patient.
In its simplest form, video or 2D gait analysis observes the movement of the lower limbs in video footages of the person walking. However observations, and interpretations, derived from video footages are limited to the sagittal and coronal planes. It may also be difficult to understand timing issues and cross-plane interactions from video footages. These limitations are addressed by 3D gait analysis which uses motion capture systems to track the movement of the lower limbs. Three-D gait analysis measures, with a high degree of accuracy, the kinematics of the joints in the lower limb and facilitates the interpretation of kinematic deviations [3, 4]. In addition, kinematics data support overall indices to qualify the gait pattern of the patient, for example some indices measure the distance to normal kinematics [5], others classify patients according to typical features [6] or measure the consistency of the gait pattern [7].
However, planning orthopaedic surgery requires more than observing and quantifying the kinematics. It requires interpretation to determine and explain the causes of the difficulties to walk so that surgery address these causes and ultimately improves the capacity of the patient to walk. The musculoskeletal system is complex and its interaction with the neuromuscular system to achieve walking is even more. With kinematics only, interpretation from gait analysis requires many conjectures and experience to relate the observed abnormal pattern to the possible causes. With the addition of measurements from force plates, 3D gait analysis calculate kinetics of the joints of the lower limb which helps lift some of the conjectures required to interpret the gait data. For example, lack of knee flexion in early stance can be linked to quad avoidance, or pain at the knee, when there is also lack of knee extensor moment. Another example is excessive coronal plane trunk kinematics, Trendelenburg gait, which is linked to weakness of the hip abductors when it is concomitant to a decreased hip abductor moment. Electrical activity of the muscles (EMG) may be acquired as well and used to explain relationships between the observed kinematics and the neural command. For example abnormal activation of the rectus femoris in late stance / early swing may be the cause of reduced peak knee flexion in swing and linked to muscle spasticity. Regrettably, EMG data only provide qualitative information about muscle activations, let alone muscle forces. Three-D gait analysis including kinetics and EMG data is able to explain most kinematic deviations when these are markedly different from the normal pattern, for example in children with cerebral palsy.
When there are no major differences in the kinematics, does it mean the patient has no problem?
Typically developing children are increasingly referred to our gait analysis service for hip or knee pain and patella mal-tracking. Often these patients exhibit large torsional deformities in the femur or tibia but sometimes do not exhibit large anomalies in the kinematic or the kinetic data. Yet the symptoms, mostly pain, are real.
To understand these symptoms and explain their causes, 3D gait analysis needs to advance and transition from data acquired from outside of the body (kinematics, kinetics and EMG) to data acquired from inside the body such as muscle forces and joint contact forces. Unfortunately there are limited means to acquire data non-invasively from inside the body. Musculoskeletal modelling provides a means to calculate these data and there are now robust open-source or commercial software packages capable of determining muscle and joint contact forces through inverse or forward dynamics calculations [8, 9]. In addition, the patient-specific neural-command, somewhat obtained from acquisition of EMG data, may now form a part of the optimisation process [10].
There are however, large challenges and limitations to the use of musculoskeletal modelling in the clinical setting. The challenges are related to the creation of patient-specific models in the clinical setting. Although these may seem trivial at first, they may also be the most difficult to solve because the biggest problems are time and cost. In fact the phrase ‘in the clinical setting’ really means ‘at most a fraction more costly than current cost and at most a fraction more time consuming than current time’, with ‘fraction’ being anything between 0 and 20%. For example, workflows based on MRI images exist to obtain accurate patient-specific anatomy, in particular for the patients with torsional deformities mentioned above. However, these involve MRI acquisitions lasting for more than 30 minutes and several hours’ segmentation and ad hoc model creation. At the moment these are clearly not adapted to our definition of clinical setting. One initiative, The Musculoskeletal Atlas Project may soon provide a solution to reduce the time required to generate ad hoc models [11]. However, the problem of access to an MRI scanner and cost of MRI acquisitions for gait analysis may still remain.
Two relatively new technologies may be adapted to the clinical setting. The first technology is freehand 3D ultrasound which combines ultrasound imaging with motion capture in order to locate the ultrasound images in space. In biomechanics, freehand 3D ultrasound has been used to measure muscle properties, e.g. volume and fascicle length [12], to measure femur torsion [13] and to locate the hip joint centre (HJC) or knee joint axis [14, 15]. The main advantages of freehand 3D ultrasound is its relatively inexpensive cost, its small dimensions and ease of transportation, leading to its availability within the gait laboratory. The drawback of freehand 3D ultrasound is the additional time required to capture and process the data, approximately 20 minutes for both HJC, 20 minutes for both femur torsion and approximately 10 minutes for both knee axes.
The second technology is EOS, a bi-plane x-ray imaging system and its associated 3D modelling software sterEOS. EOS captures two ultra-low-dose x-ray images in the sagittal and coronal planes of the whole body, or just the lower limb, while the subject is standing. From the two images, the sterEOS software allows reconstruction of the pelvis, femur and tibia shape in 3D and the software outputs all the key clinical parameters that describe the shape of these bones [16]. The main advantages of EOS are fast acquisitions, about 10 seconds to obtain the full lower limbs in the two planes, reasonable time to process data, and about 20 minutes for the pelvis, the two femurs and the two tibias. The drawback of EOS is the cost of the device and the infrastructure it requires, although EOS may be used for a range of imaging from traditional x-ray imaging to 3D modelling of the spine in patients with scoliosis.
Compared to MRI-based workflows, these two technologies have obvious limitations but they also present one critical advantage. They provide accurate information about the position of the bones with respect to the markers used in gait analysis, in the standing posture that correspond to static calibration in gait analysis [17]. This is essential to ensure accurate bone-markers registration, non-uniform scaling and deformation of the generic musculoskeletal model in order to obtain models with patient-specific anatomy.
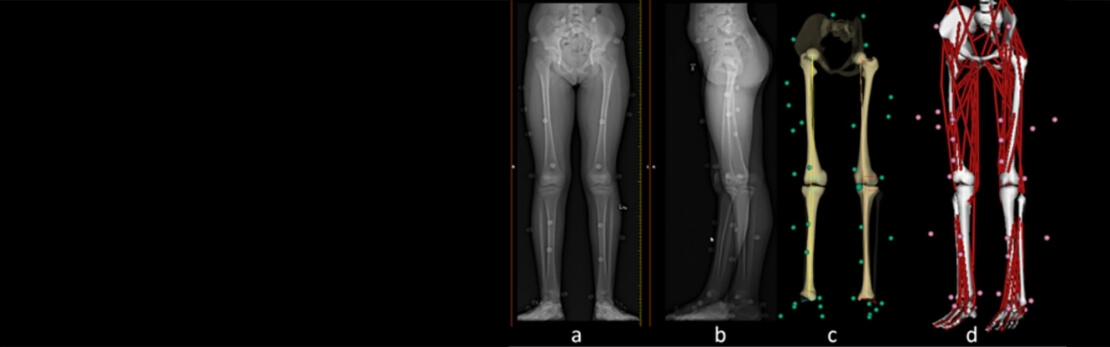
The Royal Children’s Hospital in Melbourne was equipped with an EOS system in 2014. We are developing the pipelines required to merge the EOS-derived patient-specific anatomy and the accurate bone-markers registration with the gait analysis data we collect in Nexus from our VICON system (Figure 1). This allows us to output the muscle and joint contact forces in addition to kinematics and kinetics data and facilitates the interpretation of gait analysis and surgical planning for typically developing children with torsional deformities [18].
Several challenges remain before musculoskeletal models may assist surgical planning in children with cerebral palsy. For example, the integration of patient-specific muscle properties is probably the most imperative, improved techniques and workflows to determine tendon slack length, fascicle length and maximal isometric force in the clinical setting are essential.
References
1. Lee EH, Goh JC, Bose K. Value of gait analysis in the assessment of surgery in cerebral palsy. Arch Phys Med Rehabil. 1992;73(7):642-6.
2. Chang FM, Seidl AJ, Muthusamy K, Meininger AK, Carollo JJ. Effectiveness of instrumented gait analysis in children with cerebral palsy–comparison of outcomes. J Pediatr Orthop. 2006;26(5):612-6.
3. Sangeux M, Armand S. Kinematic Deviations in Children with Cerebral Palsy In: Canavese F, Deslandes J, editors. Orthopedic Management of Children with Cerebral Palsy: A Comprehensive Approach: Nova Science Publishers; 2015.
4. Sangeux M, Passmore E, Gomez G, Balakumar J, Graham HK. Slipped capital femoral epiphysis, fixation by single screw in situ: A kinematic and radiographic study. Clin Biomech (Bristol, Avon). 2014;29(5):523-30.
5. Baker R, McGinley JL, Schwartz MH, Beynon S, Rozumalski A, Graham HK, et al. The gait profile score and movement analysis profile. Gait & Posture. 2009;30(3):265-9.
6. Sangeux M, Rodda J, Graham HK. Sagittal gait patterns in cerebral palsy: the plantarflexor-knee extension couple index. Gait & Posture. 2015;41(2):586-91.
7. Sangeux M, Passmore E, Graham HK, Tirosh O. The gait standard deviation, a single measure of kinematic variability. Gait & Posture. 2016;in press.
8. Delp SL, Anderson FC, Arnold AS, Loan P, Habib A, John CT, et al. OpenSim: open-source software to create and analyze dynamic simulations of movement. IEEE transactions on bio-medical engineering. 2007;54(11):1940-50.
9. Damsgaard M, Rasmussen J, Christensen ST, Surma E, de Zee M. Analysis of musculoskeletal systems in the AnyBody Modeling System. Simulation Modelling Practice and Theory. 2006;14(8):1100-11.
10. Pizzolato C, Lloyd DG, Sartori M, Ceseracciu E, Besier TF, Fregly BJ, et al. CEINMS: A toolbox to investigate the influence of different neural control solutions on the prediction of muscle excitation and joint moments during dynamic motor tasks. J Biomech. 2015;48(14):3929-36.
11. Zhang J, Sorby H, Clement J, Thomas C, Hunter P, Nielsen P, et al. The MAP Client: User-Friendly Musculoskeletal Modelling Workflows. In: Bello F, Cotin S, editors. Biomedical Simulation: Springer International Publishing; 2014. p. 182-92.
12. Barber L, Hastings-Ison T, Baker R, Barrett R, Lichtwark G. Medial gastrocnemius muscle volume and fascicle length in children aged 2 to 5 years with cerebral palsy. Developmental Medicine and Child Neurology. 2011;53(6):543-8.
13. Passmore E, Pandy MG, Graham HK, Sangeux M. Measuring Femoral Torsion In Vivo Using Freehand 3-D Ultrasound Imaging. Ultrasound in Medicine & Biology. 2016;42(2):619-23.
14. Sangeux M, Peters A, Baker R. Hip joint centre localization: Evaluation on normal subjects in the context of gait analysis. Gait & Posture. 2011;34(3):324-8.
15. Passmore E, Sangeux M. Defining the medial-lateral axis of an anatomical femur coordinate system using freehand 3D ultrasound imaging. Gait & Posture. 2016;45:211-6.
16. Gaumetou E, Quijano S, Ilharreborde B, Presedo A, Thoreux P, Mazda K, et al. EOS analysis of lower extremity segmental torsion in children and young adults. Orthopaedics & Traumatology, Surgery & Research : OTSR. 2014;100(1):147-51.
17. Sangeux M, Pillet H, Skalli W. Which method of hip joint centre localisation should be used in gait analysis? Gait & Posture. 2014;40(1):20-5.
18. Sangeux M, Harris C, Donnan L, Graham HK. What does it take to walk normally with high femoral neck anteversion? – A case study. 22nd Annual Meeting of the European Society for Movement Analysis in Adults and Children; Glasgow 2013.